Annual Report 2017/18 Notifications and monitoring
What's on this page
Notifications Legal services ComplianceNotifications
Performance snapshot
- 7,276 total notifications received by AHPRA in 2017/18 (up 5.5% from 2016/17) – see Figure 5
- 51.5% of notifications made to AHPRA during the year were about medical practitioners (down from 52.4% in 2016/17)
- 1.6% of all registered practitioners were the subject of a notification
- 7.2% increase in mandatory notifications made to AHPRA from 2016/17
- 68% of finalised 'immediate actions' – for matters that posed serious risk to the public – led to suspension, surrender of registration or restrictions on registration
- AHPRA closed 7,105 matters in 2017/18

An important note about our data
AHPRA does not manage all complaints made about health practitioners in Australia and our data reflect this. In this document, we are reporting mainly on matters received and managed by AHPRA and the National Boards, unless otherwise stated.
The notification process is different in NSW and Queensland:
- In NSW, AHPRA does not manage notifications. They are managed by 14 professional councils (supported by the Health Professional Councils Authority, or HPCA) and the Health Care Complaints Commission (HCCC).
- In Queensland, the Office of the Health Ombudsman (OHO) receives all complaints about health practitioners and determines which of those complaints are referred to a National Board/AHPRA to manage.
Wherever possible in the tables in this report, HPCA data are given in separate columns and the data have been checked by HPCA (correct as at time of publication). Please refer to the HPCA's 2017/18 annual report on their website, as data may have been subsequently reconciled.
Queensland became a co-regulatory jurisdiction on 1 July 2014 with the commencement of the Health Ombudsman Act. OHO receives all health complaints in Queensland, including those about registered practitioners, and decides whether the complaint:
- is serious, in which case it must be retained by OHO for investigation
- should be referred to AHPRA and the relevant National Board for management, or
- can be closed, or managed by way of conciliation or local resolution.
This means that AHPRA only has access to the data relating to matters referred to us by OHO. We do not report on all complaints about registered practitioners in Queensland. However, Tables 9 and 10 include data given to us by both HPCA and OHO.
As part of our ongoing focus to improve processes, we have continued to refine our data collection and reporting. This may mean that the data from different years may not directly correlate. For instance, since 2015/16, notifications data are based on the practitioner's principal place of practice (PPP). This is different to previous years, when data were captured based on the jurisdiction where a notification was received and managed.
For more information on how health complaints are managed in Australia, see the Performance summary.
What is a notification?
In the National Scheme, a complaint or concern about a registered health practitioner or student is called a notification.
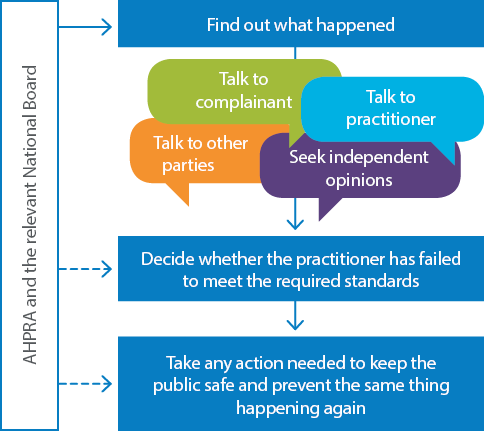
They are called notifications because we are notified about a concern or complaint, which AHPRA manages in partnership with the National Boards (refer to Figure 6). Most of the complaints and concerns we receive about individual practitioners are managed through Part 8 of the National Law. Decisions made in response to a notification can affect a practitioner's registration.
Some complaints are treated differently under the National Law, as they are considered statutory offences. AHPRA can prosecute individuals who commit these offences. For information about statutory offences in 2017/18, see below.
Keeping the public safe is our primary focus when AHPRA and the National Boards make decisions about notifications.
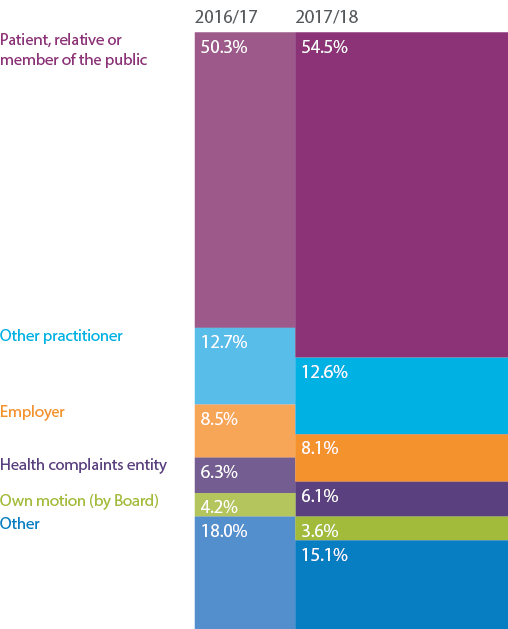
Anyone can notify us about a registered practitioner's health, performance or conduct. While registered health practitioners and employers have mandatory reporting obligations under the National Law, many of the complaints or concerns we receive are made voluntarily by patients or their families. See Figure 7.
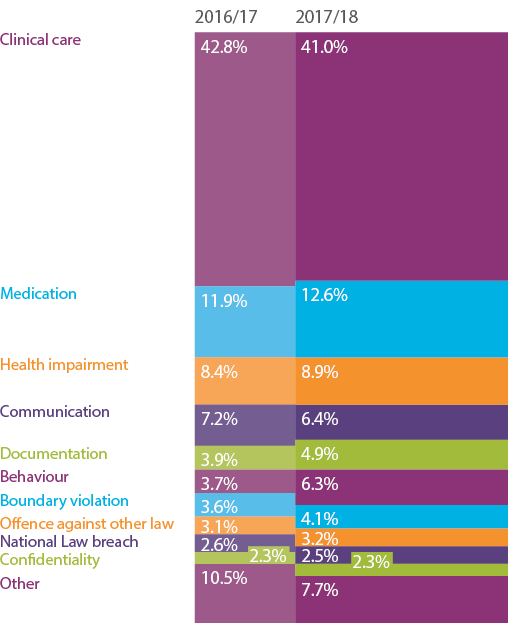
Standards of clinical care continue to be the primary issue notified to National Boards, but significant increases in volume were also recorded for behaviour and medication issues. Refer to Figure 8.
We also receive some notifications about students who are enrolled in courses that lead to eligibility for registration as a practitioner. Usually, these complaints and concerns are made by education providers or places at which students undertake clinical training. Refer to Table 12.
How we manage complaints
We are committed to ensuring that the complaints process is completed in a timely manner, taking into account the complexities of individual notifications. Every complaint or concern we receive is assessed for potential risk to the public by both AHPRA and an appropriate committee appointed by the National Boards. When our assessment concludes that we need more information, we can investigate further. When we identify that a practitioner poses a serious risk, there are interim actions that the National Boards take. Refer to Figure 9 for an outline of the notification process.

In 2017/18, AHPRA conducted a Notifications think tank to look strategically at how we manage notifications and to rethink our approach, given the growth in the number of notifications we receive. As an outcome of this think tank, AHPRA has been developing new risk-based approaches to managing notifications at assessment. This work is central to achieving timely, consistent and proportionate management of notifications, as early as possible after they are received. The work focuses on understanding the core features of regulatory risk that a notification about a practitioner might indicate. We are testing the suitability of a new risk assessment tool that cross references information received in a notification against characteristics of an individual practitioner, their individual practice circumstances and individual context of practice. Early versions of a tool for assessing regulatory risk have been piloted with some notifications committees for medical, nursing and midwifery, and dental notifications. This work will continue and increase in the next financial year, as we aim to improve approaches to managing notifications and implement the framework and risk assessment tool across all professions.
Improving the notifier and practitioner experience
Since 2016, we have been asking notifiers and practitioners to tell us about their experience of the notifications process. We have received more than 3,500 survey responses and conducted 75 in-depth interviews, aimed at understanding what is working and where we can improve. Over half of those who responded requested more information, greater transparency and regular updates. 'Fairness' emerged as a strong theme, with more than 70% of notifiers advising that they were unhappy with the outcome.
We understand that having a notification made about them can be stressful for practitioners, and this was confirmed in our survey responses with more than 90% of practitioners rating the experience as 'very stressful'. We also received significant feedback that both groups would appreciate a more personal approach, including greater telephone contact.
The information we receive from the survey is shared with staff so that they also understand the impact of our processes on the notifiers and practitioners we engage with on a daily basis. Setting a standard of what a good experience looks like is important for AHPRA and, in response to notifier and practitioner feedback, we are developing a set of experience principles based on our commitment to improving the notification experience. These include listening, informing, working in a timely way, apologising when necessary, gathering feedback and learning from it, and just and fair treatment of all notifiers and practitioners.
We will continue to focus on this work in the next year with an expectation that these experience principles will have broader application across the National Scheme.
Notifications received
This year, AHPRA received the highest number of notifications we've received in a single financial year (refer to Table 8). This equates to 7,276 notifications received, 5.5% more than the number we received in 2016/17 (6,898 notifications) and 20.1% more than in 2015/16 (6,056 notifications).
Victoria received 2,414 new notifications and Queensland received 2,079. Together, these states accounted for 61.8% of all notifications received by AHPRA in 2017/18.
In Tables 9 and 10, you will find data about practitioners with notifications made about them in 2017/18, which are segmented by the percentage of the registrant base with notifications made about them, and the number of practitioners in each profession who have had notifications made about them. These two tables not only contain AHPRA data, but data supplied to us by HPCA for NSW and OHO for Queensland.
During the year 42 students had notifications made about them to AHPRA, refer to Tables 11 and 12.
| Profession | AHPRA1 ACT |
AHPRA1 NSW2 |
AHPRA1 NT |
AHPRA1 QLD3 |
AHPRA1 SA |
AHPRA1 TAS |
AHPRA1 VIC |
AHPRA1 WA |
AHPRA1 No PPP4 |
AHPRA Subtotal 2017/18 | HPCA5 | Total 2017/18 | Total 2016/176 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 2 | 1 | 1 | 4 | 4 | 7 | |||||||
| Chinese medicine practitioner | 1 | 16 | 2 | 18 | 6 | 43 | 31 | 74 | 61 | ||||
| Chiropractor | 2 | 1 | 28 | 6 | 2 | 35 | 16 | 1 | 91 | 45 | 136 | 171 | |
| Dental practitioner | 16 | 12 | 3 | 199 | 54 | 18 | 171 | 65 | 1 | 539 | 425 | 964 | 929 |
| Medical practitioner | 121 | 63 | 69 | 1,094 | 501 | 124 | 1,203 | 544 | 30 | 3,749 | 2,599 | 6,348 | 5,913 |
| Medical radiation practitioner | 2 | 4 | 2 | 1 | 9 | 5 | 1 | 24 | 12 | 36 | 52 | ||
| Midwife | 3 | 1 | 2 | 31 | 6 | 2 | 13 | 11 | 3 | 72 | 34 | 106 | 113 |
| Nurse | 40 | 9 | 48 | 442 | 307 | 67 | 473 | 185 | 41 | 1,612 | 707 | 2,319 | 2,210 |
| Occupational therapist | 1 | 11 | 5 | 1 | 13 | 3 | 34 | 25 | 59 | 53 | |||
| Optometrist | 2 | 2 | 12 | 2 | 1 | 10 | 4 | 2 | 35 | 28 | 63 | 60 | |
| Osteopath | 1 | 2 | 13 | 1 | 17 | 15 | 32 | 25 | |||||
| Pharmacist | 2 | 5 | 3 | 127 | 33 | 17 | 204 | 46 | 14 | 451 | 312 | 763 | 645 |
| Physiotherapist | 5 | 2 | 4 | 24 | 17 | 1 | 32 | 13 | 98 | 54 | 152 | 121 | |
| Podiatrist | 1 | 3 | 17 | 3 | 2 | 24 | 9 | 2 | 61 | 27 | 88 | 61 | |
| Psychologist | 16 | 12 | 13 | 69 | 53 | 15 | 195 | 63 | 1 | 437 | 296 | 733 | 584 |
| Not identified7 | 3 | 1 | 5 | 9 | 9 | 4 | |||||||
| Total 2017/18 | 209 | 111 | 147 | 2,079 | 992 | 251 | 2,414 | 972 | 101 | 7,276 | 4,610 | 11,886 | |
| Total 2016/17 | 242 | 96 | 169 | 2,046 | 800 | 329 | 2,230 | 900 | 86 | 6,898 | 4,111 | 11,009 |
Notes:
- Based on the state or territory of the practitioner's principal place of practice.
- Matters managed by AHPRA where the conduct occurred outside NSW.
- Based on the number of matters referred by OHO to AHPRA and the National Boards.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- Matters received and managed by HPCA in NSW.
- The total for 2016/17 includes matters managed by HPCA.
- Profession of registrant is not always identifiable in the early stages of a notification.
| Profession1 | ACT | NSW2 | NT | QLD3 | SA | TAS | VIC | WA | No PPP4 | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 0.9% | 2.2% | 0.9% | 0.6% | 1.2% | ||||||
| Chinese medicine practitioner | 1.4% | 7.7% | 2.0% | 0.5% | 1.3% | 2.3% | 1.5% | 1.2% | |||
| Chiropractor | 1.4% | 2.3% | 3.7% | 3.8% | 1.6% | 2.0% | 2.1% | 2.2% | 0.6% | 2.4% | 3.1% |
| Dental practitioner | 4.3% | 4.5% | 1.8% | 5.6% | 2.3% | 3.6% | 2.7% | 2.2% | 0.2% | 3.7% | 3.8% |
| Medical practitioner | 5.4% | 5.7% | 4.3% | 7.2% | 5.4% | 4.4% | 3.6% | 4.0% | 0.7% | 5.1% | 5.1% |
| Medical radiation practitioner | 0.4% | 0.1% | 0.3% | 0.2% | 0.3% | 0.2% | 0.2% | 0.2% | 0.3% | Midwife5 | 0.4% | 0.2% | 0.5% | 0.6% | 0.2% | 0.3% | 0.2% | 0.3% | 0.0% | 0.3% | 0.3% |
| Nurse6 | 0.5% | 0.5% | 0.9% | 0.7% | 0.8% | 0.7% | 0.4% | 0.4% | 0.1% | 0.5% | 0.6% |
| Occupational therapist | 0.4% | 0.5% | 0.5% | 0.3% | 0.3% | 0.2% | 0.1% | 0.3% | 0.3% | ||
| Optometrist | 2.3% | 1.4% | 1.6% | 0.6% | 1.1% | 0.6% | 0.9% | 1.9% | 1.2% | 1.1% | |
| Osteopath | 2.6% | 2.2% | 2.8% | 1.0% | 1.6% | 1.4% | 1.1% | ||||
| Pharmacist | 0.3% | 1.9% | 1.6% | 2.4% | 1.5% | 2.0% | 2.0% | 1.4% | 0.7% | 1.9% | 1.8% |
| Physiotherapist | 0.6% | 0.5% | 2.2% | 0.6% | 0.6% | 0.2% | 0.4% | 0.3% | 0.1% | 0.5% | 0.4% |
| Podiatrist | 1.5% | 1.7% | 2.2% | 0.7% | 1.9% | 1.3% | 1.7% | 5.1% | 1.6% | 1.3% | |
| Psychologist | 1.5% | 2.0% | 4.3% | 2.1% | 2.5% | 2.1% | 1.7% | 1.5% | 0.2% | 1.9% | 1.6% |
| Total 2017/18 | 1.6% | 1.8% | 1.8% | 2.1% | 1.6% | 1.5% | 1.1% | 1.2% | 0.3% | 1.6% | |
| Total 2016/17 | 1.9% | 1.7% | 2.2% | 2.2% | 1.3% | 1.9% | 1.1% | 1.2% | 0.5% | 1.6% |
Notes:
- Percentages for each state and profession are based on registrants whose profession has been identified and whose principal place of practice (PPP) is an Australian state or territory.
- NSW data include matters managed by HPCA, as well as notifications managed by AHPRA about a practitioner with a PPP in NSW.
- Queensland data include matters managed by OHO, as well as those referred to AHPRA by OHO.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- The registrant base used for midwives includes registrants with midwifery or with nursing and midwifery registration.
- The registrant base for nurses includes registrants with nursing registration or with nursing and midwifery registration.
| Profession1 | ACT | NSW2 | NT | QLD3 | SA | TAS | VIC | WA | No PPP4 | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 2 | 1 | 1 | 4 | 7 | Chinese medicine practitioner | 28 | 1 | 18 | 1 | 17 | 6 | 71 | 60 |
| Chiropractor | 1 | 41 | 1 | 33 | 6 | 1 | 30 | 14 | 1 | 128 | 164 |
| Dental practitioner | 18 | 311 | 3 | 256 | 43 | 14 | 147 | 58 | 1 | 851 | 853 |
| Medical practitioner | 117 | 2,029 | 58 | 1,664 | 442 | 106 | 1,027 | 463 | 21 | 5,927 | 5,711 |
| Medical radiation practitioner | 1 | 7 | 10 | 2 | 1 | 8 | 3 | 32 | 48 | ||
| Midwife5 | 3 | 18 | 3 | 44 | 6 | 2 | 14 | 10 | 100 | 95 | |
| Nurse6 | 33 | 577 | 43 | 536 | 278 | 65 | 425 | 172 | 14 | 2,143 | 2,151 |
| Occupational therapist | 21 | 1 | 19 | 5 | 1 | 11 | 3 | 61 | 58 | ||
| Optometrist | 2 | 26 | 18 | 2 | 1 | 9 | 4 | 3 | 65 | 57 | |
| Osteopath | 1 | 13 | 6 | 13 | 1 | 34 | 25 | ||||
| Pharmacist | 2 | 181 | 4 | 147 | 33 | 15 | 161 | 45 | 4 | 592 | 545 |
| Physiotherapist | 4 | 51 | 4 | 39 | 16 | 1 | 29 | 12 | 1 | 157 | 133 |
| Podiatrist | 1 | 24 | 19 | 3 | 2 | 22 | 8 | 3 | 82 | 62 | |
| Psychologist | 14 | 241 | 10 | 138 | 44 | 13 | 168 | 58 | 1 | 687 | 571 |
| Total 2017/18 | 197 | 3,568 | 130 | 2,947 | 882 | 222 | 2,081 | 858 | 49 | 10,934 | |
| Total 2016/17 | 222 | 3,332 | 155 | 2,958 | 726 | 282 | 1,961 | 819 | 85 | 10,540 |
Notes:
- Numbers for each state and profession are based on registrants whose profession has been identified and whose principal place of practice (PPP) is an Australian state or territory.
- NSW data include matters managed by HPCA, as well as notifications managed by AHPRA about a practitioner with a PPP in NSW.
- Queensland data include matters managed by OHO, as well as those referred to AHPRA by OHO.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- The registrant base used for midwives includes registrants with midwifery or with nursing and midwifery registration.
- The registrant base for nurses includes registrants with nursing registration or with nursing and midwifery registration.
| Profession | AHPRA1 ACT |
AHPRA1 NSW |
AHPRA1 NT |
AHPRA1 QLD |
AHPRA1 SA |
AHPRA1 TAS |
AHPRA1 VIC |
AHPRA1 WA |
AHPRA1 No PPP2 |
AHPRA Subtotal 2017/18 | HPCA3 | Total 2017/18 | Total 2016/17 | Aboriginal and Torres Strait Islander Health Practitioner | 0 | 0 | 0 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chinese medicine practitioner | 0 | 0 | 1 | ||||||||||
| Chiropractor | 0 | 1 | 1 | 1 | |||||||||
| Dental practitioner | 1 | 1 | 2 | 3 | 1 | ||||||||
| Medical practitioner | 3 | 1 | 6 | 10 | 9 | 19 | 9 | ||||||
| Medical radiation practitioner | 0 | 1 | 1 | 2 | |||||||||
| Midwife | 1 | 1 | 4 | 6 | 1 | 7 | 0 | ||||||
| Nurse | 1 | 20 | 21 | 14 | 35 | 43 | |||||||
| Occupational therapist | 0 | 1 | 1 | 2 | |||||||||
| Optometrist | 0 | 0 | 0 | ||||||||||
| Osteopath | 0 | 3 | 3 | 1 | |||||||||
| Pharmacist | 2 | 2 | 3 | 5 | 1 | ||||||||
| Physiotherapist | 0 | 0 | 0 | ||||||||||
| Podiatrist | 2 | 2 | 1 | 3 | 1 | ||||||||
| Psychologist | 0 | 0 | 0 | ||||||||||
| Total 2017/18 | 0 | 0 | 0 | 5 | 2 | 0 | 0 | 1 | 34 | 42 | 36 | 78 | |
| Total 2016/17 | 0 | 1 | 0 | 4 | 3 | 1 | 1 | 0 | 20 | 30 | 32 | 62 |
Notes:
- Based on state and territory of the student's principal place of practice.
- No principal place of practice (No PPP) includes students with an overseas or unknown address.
- Matters received and managed by HPCA in NSW.
| Stage at closure | Assessment | Health or performance assessment |
Investigation | Panel hearing | Tribunal hearing | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|
| No further action – AHPRA | 17 | 4 | 7 | 28 | 21 | ||
| No further action – HPCA1 | 3 | 3 | 6 | 16 | |||
| Impose conditions – AHPRA | 1 | 2 | 3 | 6 | |||
| Impose conditions – HPCA | 2 | 2 | 13 | ||||
| Accept undertaking – AHPRA | 1 | 1 | 2 | 1 | |||
| Accept undertaking – HPCA | 0 | 0 | |||||
| Caution – AHPRA | 0 | 4 | |||||
| Caution – HPCA | 0 | 0 | |||||
| Cancel registration – AHPRA | 0 | 1 | |||||
| Cancel registration – HPCA | 0 | 0 | |||||
| No jurisdiction – AHPRA | 0 | 0 | |||||
| No jurisdiction – HPCA | 3 | 2 | 5 | 5 | |||
| Refer to other entity – AHPRA | 0 | 0 | |||||
| Refer to other entity – HPCA | 2 | 2 | 1 | ||||
| Discontinue – AHPRA | 0 | 0 | |||||
| Discontinue – HPCA | 7 | 7 | 3 | ||||
| Counselling – AHPRA | 0 | 0 | |||||
| Counselling – HPCA | 0 | 0 | |||||
| Surrender – AHPRA | 0 | 0 | |||||
| Surrender – HPCA | 0 | 1 | |||||
| Withdrawn – AHPRA | 0 | 0 | |||||
| Withdrawn – HPCA | 0 | 1 | |||||
| Total 2017/18 | 34 | 9 | 8 | 4 | 0 | 55 | |
| Total 2016/17 | 32 | 11 | 11 | 18 | 1 | 73 |
Notes:
- Matters managed by HPCA in NSW.
Mandatory notifications
All health practitioners, their employers and education providers have mandatory reporting responsibilities under
the National Law.
This means that they must tell AHPRA if they have formed a reasonable belief that a registered practitioner or student has behaved in a way that constitutes notifiable conduct.
Notifiable conduct by registered practitioners is defined as:
- practising while intoxicated by alcohol or drugs
- engaging in sexual misconduct in the practice of the profession
- placing the public at risk of substantial harm because of an impairment (health issue), or
- placing the public at risk because of a significant departure from accepted professional standards.
AHPRA received 908 mandatory notifications in 2017/18, up by 7.2% (61 notifications) compared with 2016/17. More than 79.5% of the mandatory notifications received were about medical practitioners or nurses, which is consistent with long-term trends. Almost 45% of mandatory notifications completed during 2017/18 resulted in some form of regulatory action being taken against a practitioner. This is consistent with trends from previous years and suggests a continued understanding of the mandatory notification requirements under the National Law. Notifiers are making appropriate mandatory notifications, having reasonably assessed that the risk to the public warrants the notification being made. Refer to Tables 13, 14 and 15.
| Profession | AHPRA1 ACT |
AHPRA1 NSW2 |
AHPRA1 NT |
AHPRA1 QLD3 |
AHPRA1 SA |
AHPRA1 TAS |
AHPRA1 VIC |
AHPRA1 WA |
AHPRA1 No PPP4 |
AHPRA Subtotal 2017/18 | HPCA5 | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 1 | 1 | 2 | 2 | 2 | ||||||||
| Chinese medicine practitioner | 1 | 2 | 3 | 3 | 1 | ||||||||
| Chiropractor | 1 | 3 | 2 | 6 | 2 | 8 | 15 | ||||||
| Dental practitioner | 2 | 12 | 15 | 2 | 31 | 31 | 29 | ||||||
| Medical practitioner | 13 | 7 | 12 | 4 | 50 | 10 | 116 | 38 | 5 | 255 | 88 | 343 | 294 |
| Medical radiation practitioner | 1 | 1 | 3 | 3 | 8 | 8 | 8 | ||||||
| Midwife | 1 | 2 | 1 | 4 | 8 | 14 | 22 | 21 | |||||
| Nurse | 8 | 4 | 12 | 2 | 165 | 22 | 172 | 68 | 14 | 467 | 234 | 701 | 639 |
| Occupational therapist | 2 | 3 | 2 | 7 | 3 | 10 | 6 | ||||||
| Optometrist | 1 | 1 | 2 | 2 | 4 | 1 | |||||||
| Osteopath | 1 | 1 | 1 | 2 | 1 | ||||||||
| Pharmacist | 1 | 1 | 1 | 9 | 4 | 24 | 2 | 2 | 44 | 4 | 48 | 65 | |
| Physiotherapist | 4 | 8 | 5 | 17 | 4 | 21 | 12 | ||||||
| Podiatrist | 2 | 2 | 1 | 5 | 2 | 7 | 5 | ||||||
| Psychologist | 6 | 2 | 13 | 3 | 22 | 6 | 52 | 8 | 60 | 43 | |||
| Total 2017/18 | 28 | 17 | 27 | 8 | 260 | 42 | 372 | 132 | 22 | 908 | 362 | 1,270 | |
| Total 2016/17 | 32 | 7 | 15 | 13 | 255 | 73 | 335 | 111 | 6 | 847 | 295 | 1,142 |
- Based on state and territory of the practitioner's principal place of practice.
- Matters managed by AHPRA where the conduct occurred outside NSW.
- Based on the number of matters referred by OHO to AHPRA and the National Boards.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- Mandatory notifications received and managed by HPCA in NSW.
| Profession | Standards – AHPRA | Standards – HPCA1 | Impairment – AHPRA | Impairment – HPCA | Alcohol or drugs –AHPRA | Alcohol or drugs – HPCA | Sexual misconduct –AHPRA | Sexual misconduct – HPCA | Total 2017/18 – AHPRA | Total 2017/18 – HPCA | Total 2016/17 – AHPRA | Total 2016/17 – HPCA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 2 | 2 | 0 | 2 | 0 | |||||||
| Chinese medicine practitioner | 3 | 3 | 0 | 0 | 1 | |||||||
| Chiropractor | 6 | 2 | 6 | 2 | 11 | 4 | ||||||
| Dental practitioner | 27 | 3 | 1 | 31 | 0 | 21 | 8 | |||||
| Medical practitioner | 188 | 53 | 43 | 20 | 5 | 4 | 19 | 11 | 255 | 88 | 224 | 70 |
| Medical radiation practitioner | 5 | 2 | 1 | 8 | 0 | 6 | 2 | |||||
| Midwife | 6 | 12 | 2 | 2 | 8 | 14 | 17 | 4 | ||||
| Nurse | 330 | 156 | 93 | 76 | 31 | 13 | 2 | 467 | 234 | 471 | 168 | |
| Occupational therapist | 4 | 1 | 2 | 3 | 7 | 3 | 4 | 2 | ||||
| Optometrist | 2 | 1 | 1 | 2 | 2 | 1 | 0 | |||||
| Osteopath | 1 | 1 | 1 | 1 | 0 | 1 | ||||||
| Pharmacist | 36 | 4 | 7 | 1 | 44 | 4 | 51 | 14 | ||||
| Physiotherapist | 12 | 1 | 2 | 1 | 1 | 2 | 2 | 17 | 4 | 8 | 4 | |
| Podiatrist | 2 | 1 | 2 | 1 | 1 | 5 | 2 | 4 | 1 | |||
| Psychologist | 35 | 5 | 11 | 3 | 6 | 52 | 8 | 27 | 16 | |||
| Total 2017/18 | 656 | 233 | 167 | 105 | 42 | 5 | 43 | 19 | 908 | 362 | ||
Total 2016/17
| 619 |
173 |
148 |
72 |
34 |
29 |
46 |
21 |
|
|
847 |
295 |
|
Notes:
- Matters managed by HPCA in NSW.
| Profession | Aboriginal and Torres Strait Islander Health Practitioner | Chinese medicine practitioner | Chiropractor | Dental practitioner | Medical practitioner | Medical radiation practitioner | Midwife | Nurse | Occupational therapist | Optometrist | Osteopath | Pharmacist | Physiotherapist | Podiatrist | Psychologist | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Discontinued/proceedings withdrawn – AHPRA | 0 | 0 | |||||||||||||||
| Discontinued/proceedings withdrawn – HPCA | 20 | 16 | 1 | 1 | 1 | 1 | 40 | 30 | |||||||||
| Changed to non-practising – AHPRA | 0 | 0 | |||||||||||||||
| Changed to non-practising – HPCA | 0 | 3 | |||||||||||||||
| Other/no jurisdiction – AHPRA | 0 | 0 | |||||||||||||||
| Other/no jurisdiction – HPCA1 | 1 | 2 | 28 | 31 | 19 | ||||||||||||
| Counselling – AHPRA | 0 | 0 | |||||||||||||||
| Counselling – HPCA | 1 | 30 | 2 | 33 | 23 | ||||||||||||
| No further action – AHPRA | 1 | 5 | 21 | 147 | 1 | 8 | 238 | 3 | 2 | 18 | 4 | 2 | 27 | 477 | 408 | ||
| No further action – HPCA | 18 | 2 | 64 | 1 | 3 | 88 | 127 | ||||||||||
| Refer all or part of the notification to another body – AHPRA | 6 | 2 | 1 | 1 | 10 | 4 | |||||||||||
| Refer all or part of the notification to another body – HPCA | 4 | 1 | 5 | 10 | |||||||||||||
| Fine registrant – AHPRA | 3 | 3 | 4 | ||||||||||||||
| Fine registrant – HPCA | 0 | 0 | |||||||||||||||
| Orders – no conditions – AHPRA | 0 | 0 | |||||||||||||||
| Orders – no conditions – HPCA | 1 | 1 | 2 | ||||||||||||||
| Caution or reprimand – AHPRA | 2 | 2 | 27 | 1 | 1 | 64 | 2 | 18 | 1 | 2 | 120 | 142 | |||||
| Caution or reprimand – HPCA | 3 | 4 | 3 | 10 | 3 | ||||||||||||
| Accept undertaking – AHPRA | 1 | 16 | 38 | 3 | 58 | 52 | |||||||||||
| Accept undertaking – HPCA | 0 | 0 | |||||||||||||||
| Impose conditions – AHPRA | 1 | 7 | 28 | 2 | 6 | 98 | 1 | 14 | 5 | 1 | 13 | 176 | 152 | ||||
| Impose conditions – HPCA2 | 2 | 2 | 15 | 36 | 3 | 1 | 3 | 62 | 65 | ||||||||
| Accept surrender of registration – AHPRA | 0 | 2 | |||||||||||||||
| Accept surrender of registration – HPCA | 2 | 2 | 9 | ||||||||||||||
| Suspend registration – AHPRA | 5 | 6 | 11 | 10 | |||||||||||||
| Suspend registration – HPCA | 1 | 3 | 4 | 1 | |||||||||||||
| Cancel registration/disqualify – AHPRA | 4 | 2 | 6 | 18 | |||||||||||||
| Cancel registration/disqualify – HPCA | 3 | 6 | 1 | 1 | 11 | 10 | |||||||||||
| Not permitted to reapply for registration for 12 months or more – AHPRA | 0 | 0 | |||||||||||||||
| Not permitted to reapply for registration for 12 months or more – HPCA | 0 | 0 | |||||||||||||||
| Total 2017/18 – AHPRA | 2 | 0 | 7 | 31 | 236 | 4 | 15 | 448 | 7 | 2 | 0 | 54 | 10 | 3 | 42 | 861 | |
| Total 2017/18 – HPCA | 0 | 0 | 2 | 2 | 68 | 0 | 5 | 188 | 0 | 0 | 1 | 4 | 4 | 2 | 11 | 287 | |
| Total 2016/17 – AHPRA | 1 | 2 | 12 | 25 | 221 | 6 | 19 | 426 | 2 | 0 | 0 | 42 | 5 | 4 | 27 | 792 | |
| Total 2016/17 – HPCA | 0 | 2 | 1 | 4 | 66 | 4 | 0 | 177 | 2 | 0 | 2 | 12 | 4 | 1 | 27 | 302 |
Notes:
- Includes practitioners who failed to renew.
- Includes conditions by consent.
Immediate action
Immediate action is a serious step that a National Board can take when it believes it is necessary to limit a practitioner's registration in some way to keep the public safe.
It is an interim measure that a Board takes only in cases where the Board believes there is a serious risk to the public or it is otherwise in the public interest to limit a practitioner's registration while it seeks further information.
In 2017/18, National Boards took immediate action on 413 occasions, which is 29.4% (320) more than in 2016/17. The proportion of notifications where immediate action was taken was 5.7% of the notifications received. This is relatively consistent with previous years (4.6% in 2016/17 and 6.2% in 2015/16). Refer to Table 16 for the breakdown of immediate action taken over the last three years and Table 17 for the breakdown by profession in 2017/18.
Timeliness in managing risk is crucial when dealing with a matter where immediate action may be required. The median time to take immediate action was seven days in 2017/18, which is the same as it was in 2016/17. In 2015/16 it was eight days. The median time continues to compare favourably to health practitioner regulators in the United Kingdom.
The multi-profession immediate action approach of nine National Boards continued this year. A new, single immediate action committee for the Psychology Board of Australia was also introduced (previously, each regional board of the Psychology Board of Australia managed immediate actions).
See the appendices in this report for information about meetings of these committees. For more information about our work on cross-profession collaboration, see Multi-profession policy.
| Type of immediate action taken | 2015/16 | 2016/17 | 2017/18 |
|---|---|---|---|
| Registration surrendered | 1.6% | 0.3% | 0.2% |
| Accept undertaking | 17.8% | 21.6% | 27.3% |
| Impose conditions | 60.9% | 45.9% | 42.0% |
| Suspended | 19.7% | 32.2% | 30.4% |
| Profession | No action taken AHPRA |
No action taken HPCA3,4 |
Action taken1 Suspend registration AHPRA |
Action taken1 Suspend registration HPCA |
Action taken1 Accept surrender of registration AHPRA |
Action taken1 Accept surrender of registration HPCA |
Action taken1 Impose conditions AHPRA |
Action taken1 Impose conditions HPCA |
Action taken1 Accept undertaking AHPRA |
Action taken1 Accept undertaking HPCA |
Decision pending2 AHPRA |
Decision pending2 HPCA |
Total 2017/18 AHPRA |
Total 2017/18 HPCA |
Total 2016/17 AHPRA |
Total 2016/17 HPCA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 1 | 1 | 2 | 0 | 0 | 0 | ||||||||||
| Chinese medicine practitioner | 1 | 2 | 1 | 3 | 6 | 1 | 1 | 1 | ||||||||
| Chiropractor | 4 | 1 | 2 | 3 | 2 | 1 | 2 | 10 | 5 | 15 | 5 | |||||
| Dental practitioner | 6 | 1 | 4 | 6 | 2 | 11 | 4 | 1 | 17 | 18 | 15 | 17 | ||||
| Medical practitioner | 76 | 19 | 32 | 20 | 5 | 65 | 70 | 51 | 8 | 4 | 232 | 118 | 160 | 91 | ||
| Medical radiation practitioner | 1 | 1 | 1 | 3 | 0 | 2 | 2 | |||||||||
| Midwife | 2 | 3 | 1 | 2 | 2 | 5 | 10 | 5 | 4 | 1 | ||||||
| Nurse | 67 | 43 | 64 | 11 | 1 | 85 | 94 | 42 | 10 | 269 | 148 | 182 | 92 | |||
| Occupational therapist | 1 | 1 | 2 | 1 | 1 | 4 | 2 | 0 | 0 | |||||||
| Optometrist | 1 | 1 | 0 | 2 | 2 | 0 | ||||||||||
| Osteopath | 2 | 1 | 3 | 0 | 1 | 2 | ||||||||||
| Pharmacist | 1 | 8 | 4 | 4 | 7 | 27 | 4 | 1 | 17 | 39 | 22 | 49 | ||||
| Physiotherapist | 8 | 3 | 3 | 1 | 2 | 1 | 13 | 5 | 1 | 2 | ||||||
| Podiatrist | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| Psychologist | 3 | 2 | 11 | 3 | 4 | 7 | 3 | 1 | 22 | 12 | 13 | 9 | ||||
| Total 2017/18 | 173 | 80 | 126 | 50 | 1 | 5 | 174 | 217 | 113 | 0 | 22 | 4 | 609 | 356 | ||
| Total 2016/17 | 76 | 63 | 103 | 42 | 1 | 0 | 147 | 167 | 69 | 0 | 23 | 0 | 419 | 272 |
Notes:
- Cases where immediate action has been initiated under Part 8, Division 7 of the National Law.
- In these cases where immediate action was initiated towards the close of the reporting year, an outcome decision has not been finalised.
- Matters managed by HPCA in NSW.
- HPCA data exclude matters that were considered for immediate action but did not proceed to a hearing, other than matters where the case did not proceed because the practitioner surrendered registration.
Investigations
Sometimes, the information available to a National Board when assessing a complaint or concern is not sufficient to enable a risk-informed decision. In these cases, a National Board can conduct an investigation to gather more information that is relevant to the case. A decision to investigate is not an indication that a National Board has accepted an allegation made in a notification as true.
During an investigation, information can be gathered from sources such as:
- the person who raised their concern with the Board (the notifier)
- the practitioner being investigated
- contents of patient records
- other practitioners who may have been involved in the care of a patient
- witnesses (for example, family members, other patients or staff members)
- experts (who provide independent opinions) or information from professional bodies
- police reports, and/or
- information from other sources such as pharmacy records, health insurers or Medicare Australia.
In 2017/18, National Boards began 2,598 investigations; 5.1% more than in the previous year. Despite the increased volume of notifications, the proportion that progressed to investigation was largely consistent with previous years at 33.0%, compared to 33.2% in 2016/17 and 36.4% in 2015/16.
In addition to regular updates on the progress of individual investigations, AHPRA routinely audits older investigations as a quality-assurance mechanism to identify ways we can reduce the time it takes for AHPRA and the Boards to investigate matters. This year, AHPRA began an investigation case conferencing project that:
- aims to review and reduce aged investigations
- identifies what issues or incidents during the lifecycle of an investigation are contributing to the time taken to complete the investigation
- considers whether clinical input can be better utilised during investigation, and
- will inform our ongoing work on assessing risk by identifying common types of information that can indicate that an investigation is likely to result in a decision to take no regulatory action.
The findings of the project will be assessed and applied to determine what activities may be introduced (or removed) to reduce the likelihood of investigations becoming aged. This work will continue into the next financial year.
We continue to refine processes to ensure timely outcomes for notifiers and practitioners, and have reduced the average number of days to complete an investigation from 398 in 2015/16, to 392 in 2016/17 and 379 days in 2017/18.
Outcomes and timeliness of notifications closed
We assessed and completed 6.5% more notifications in 2017/18 than in 2016/17. This represents the highest number of closures (7,105) since the start of the National Scheme. Of notifications that were closed, 27.8% resulted in some form of regulatory action being taken by a National Board (refer to Table 18).
The average time taken to complete an assessment and to close matters in assessment is shown in Table 19.
Table 20 shows notifications closed by profession and stage at closure and Table 21 by profession and outcome, while Table 22 contains data provided to us by HPCA about notifications closed in NSW.
Tables 23 and 24 contain data about 4,187 notifications that are currently being managed by AHPRA and remained open as at 30 June 2018.
The average time taken to close a notification in 2017/18 is shown in Figure 10. The majority (64.5%) closed in six months, which is consistent with previous years (64.9% in 2016/17 and 64.0% in 2015/16).
| Closed notification outcomes | 2015/16 | 2016/17 | 2017/18 |
|---|---|---|---|
| No further action | 66.5% | 68.6% | 72.0% |
| Caution or reprimand | 13.8% | 14.2% | 11.5% |
| Impose conditions | 11.1% | 10.6% | 9.7% |
| Accept undertaking | 3.5% | 2.2% | 2.2% |
| Refer to a HCE or other entity | 3.3% | 3.2% | 3.4% |
| Registration surrendered, suspended or cancelled | 1.9% | 1.2% | 1.0% |
| Average time (in days) to: | 2015/16 | 2016/17 | 2017/18 | % change 2016/17–2017/18 |
|---|---|---|---|---|
| Close matters in assessment | 82 | 84 | 82 | -2.4% |
| Complete assessments and move to another stage | 48 | 51 | 42 | -17.6% |
Changes to the process for assessing notifications about medical practitioners and medical students through 2017/18 led to a 26.1% reduction in the time taken to assess notifications. Medical assessments are completed in 51 days on average; 23.9% better than the national 'all boards' result of 67 days.
The final step in implementing the new process approach for medical notifications is to incorporate Tasmanian and ACT medical notifications and this will be completed in 2018.

| Profession | Assessment – AHPRA | Assessment – HPCA1 | Investigation – AHPRA | Investigation – HPCA | Health or performance assessment – AHPRA | Health or performance assessment – HPCA | Panel hearing – AHPRA | Panel hearing – HPCA | Tribunal hearing – AHPRA | Tribunal hearing – HPCA2 | Subtotal 2017/18 – AHPRA | Subtotal 2017/18 – HPCA | Total 2017/18 | Total 2016/17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 2 | 1 | 1 | 4 | 0 | 4 | 6 | ||||||||
| Chinese medicine practitioner | 25 | 40 | 3 | 1 | 1 | 1 | 30 | 41 | 71 | 65 | |||||
| Chiropractor | 46 | 58 | 44 | 3 | 2 | 1 | 2 | 26 | 2 | 120 | 64 | 184 | 152 | ||
| Dental practitioner | 379 | 358 | 144 | 1 | 22 | 27 | 3 | 54 | 6 | 3 | 554 | 443 | 997 | 871 | |
| Medical practitioner | 2,435 | 1,713 | 1,055 | 93 | 119 | 376 | 16 | 96 | 78 | 35 | 3,703 | 2,313 | 6,016 | 5,654 | |
| Medical radiation practitioner | 13 | 16 | 5 | 1 | 5 | 1 | 2 | 1 | 24 | 20 | 44 | 49 | |||
| Midwife | 45 | 9 | 27 | 6 | 12 | 1 | 1 | 1 | 80 | 22 | 102 | 135 | |||
| Nurse | 803 | 476 | 497 | 17 | 230 | 30 | 13 | 87 | 37 | 17 | 1,580 | 627 | 2,207 | 2,050 | |
| Occupational therapist | 25 | 17 | 6 | 2 | 3 | 1 | 34 | 20 | 54 | 55 | |||||
| Optometrist | 22 | 24 | 9 | 1 | 5 | 32 | 29 | 61 | 50 | ||||||
| Osteopath | 11 | 16 | 6 | 3 | 1 | 17 | 20 | 37 | 18 | ||||||
| Pharmacist | 272 | 246 | 109 | 15 | 12 | 6 | 40 | 9 | 5 | 411 | 303 | 714 | 572 | ||
| Physiotherapist | 50 | 54 | 28 | 3 | 3 | 1 | 1 | 82 | 58 | 140 | 116 | ||||
| Podiatrist | 28 | 20 | 12 | 1 | 41 | 20 | 61 | 70 | |||||||
| Psychologist | 264 | 235 | 93 | 9 | 13 | 6 | 8 | 9 | 4 | 381 | 260 | 641 | 547 | ||
| Not identified3 | 11 | 1 | 12 | 0 | 12 | 3 | |||||||||
| Total 2017/18 | 4,431 | 3,282 | 2,039 | 112 | 419 | 480 | 47 | 297 | 169 | 69 | 7,105 | 4,240 | 11,345 | ||
| Total 2016/17 | 4,141 | 3,145 | 1,919 | 62 | 362 | 188 | 72 | 293 | 175 | 56 | 6,669 | 3,744 | 10,413 |
Notes:
- Matters managed by HPCA in NSW.
- Excludes appeals.
- Practitioner profession may not have been identified in notifications closed at an early stage.
| Profession | No further action | Refer all or part of the notification to another body | HCE to retain1 | Accept undertaking | Caution or reprimand | Fine registrant | Impose conditions | Accept surrender of registration | Suspend registration | Cancel registration | Not permitted to reapply for registration for 12 months or more | Total 2017/182 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 3 | 1 | 4 | 6 | |||||||||
| Chinese medicine practitioner | 25 | 1 | 3 | 1 | 30 | 34 | |||||||
| Chiropractor | 53 | 25 | 1 | 26 | 13 | 2 | 120 | 88 | |||||
| Dental practitioner | 368 | 6 | 15 | 13 | 79 | 72 | 1 | 554 | 485 | ||||
| Medical practitioner | 2,970 | 23 | 128 | 64 | 249 | 8 | 225 | 16 | 20 | 3,703 | 3,557 | ||
| Medical radiation practitioner | 14 | 4 | 6 | 24 | 29 | ||||||||
| Midwife | 47 | 2 | 16 | 15 | 80 | 86 | |||||||
| Nurse | 984 | 11 | 23 | 58 | 245 | 2 | 231 | 5 | 15 | 6 | 1,580 | 1,473 | |
| Occupational therapist | 19 | 2 | 1 | 9 | 1 | 2 | 34 | 39 | |||||
| Optometrist | 21 | 2 | 4 | 5 | 32 | 27 | |||||||
| Osteopath | 13 | 2 | 1 | 1 | 17 | 13 | |||||||
| Pharmacist | 225 | 3 | 1 | 10 | 122 | 1 | 48 | 1 | 411 | 355 | |||
| Physiotherapist | 46 | 2 | 3 | 14 | 17 | 82 | 83 | ||||||
| Podiatrist | 27 | 1 | 7 | 6 | 41 | 47 | |||||||
| Psychologist | 291 | 1 | 1 | 3 | 39 | 41 | 4 | 1 | 381 | 344 | |||
| Not identified | 10 | 2 | 12 | 3 | |||||||||
| Total 2017/18 | 5,116 | 71 | 174 | 158 | 816 | 12 | 686 | 5 | 37 | 30 | 0 | 7,105 | |
| Total 2016/17 | 4,572 | 54 | 159 | 149 | 946 | 11 | 706 | 5 | 30 | 34 | 3 | 6,669 |
Notes:
- Health complaints entity.
- A matter may result in more than one outcome. Only the most serious outcome from each closed notification has been noted.
| Profession | Aboriginal and Torres Strait Islander Health Practitioner |
Chinese medicine practitioner | Chiropractor | Dental practitioner | Medical practitioner | Medical radiation practitioner | Midwife | Nurse | Occupational therapist | Optometrist | Osteopath | Pharmacist | Physiotherapist | Podiatrist | Psychologist | Total 2017/18 | Total 2016/17 | No further action1 | 17 | 24 | 93 | 386 | 5 | 10 | 194 | 7 | 12 | 2 | 120 | 6 | 10 | 67 | 953 | 1,108 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No jurisdiction2 | 5 | 4 | 29 | 1 | 2 | 63 | 1 | 4 | 4 | 16 | 129 | 77 | |||||
| Discontinued | 8 | 16 | 201 | 1,604 | 9 | 6 | 189 | 12 | 16 | 6 | 118 | 31 | 9 | 133 | 2,358 | 1,906 | |
| Withdrawn | 1 | 7 | 42 | 2 | 4 | 2 | 8 | 66 | 78 | ||||||||
| Make a new complaint | 0 | 0 | |||||||||||||||
| Refer all or part of the notification to another body | 6 | 14 | 27 | 85 | 2 | 1 | 11 | 1 | 5 | 4 | 10 | 1 | 16 | 181 | 119 | ||
| Caution | 29 | 1 | 7 | 37 | 18 | ||||||||||||
| Reprimand | 1 | 1 | 12 | 6 | 3 | 4 | 27 | 30 | |||||||||
| Orders – no conditions | 6 | 2 | 8 | 13 | |||||||||||||
| Finding – no orders | 1 | 1 | 3 | 5 | 2 | ||||||||||||
| Counselling/interview | 4 | 4 | 50 | 16 | 3 | 91 | 2 | 16 | 5 | 6 | 197 | 114 | |||||
| Resolution/conciliation by HCCC | 1 | 31 | 32 | 18 | |||||||||||||
| Fine | 0 | 0 | |||||||||||||||
| Refund/payment/withhold fee/retreat | 0 | 0 | |||||||||||||||
| Conditions by consent | 25 | 43 | 3 | 71 | 66 | ||||||||||||
| Order – impose conditions; would be conditions if registered | 1 | 3 | 36 | 40 | 2 | 22 | 1 | 23 | 3 | 10 | 141 | 151 | |||||
| Accept surrender | 3 | 16 | 19 | 32 | |||||||||||||
| Accept registration type change to non-practising | 1 | 1 | 2 | 7 | |||||||||||||
| Suspend | 3 | 3 | 6 | 5 | |||||||||||||
| Cancelled registration/disqualified from registering | 1 | 11 | 28 | 1 | 11 | 4 | 1 | 3 | 60 | 53 | |||||||
| Total 2017/18 | 0 | 41 | 65 | 469 | 2,322 | 20 | 22 | 633 | 20 | 29 | 20 | 309 | 58 | 20 | 264 | 4,292 | |
| Total 2016/17 | 0 | 32 | 65 | 406 | 2,111 | 20 | 49 | 586 | 16 | 23 | 5 | 225 | 33 | 23 | 203 | 3,797 |
Source: The data in this table were supplied by the Health Professional Councils Authority (HPCA). NSW legislation provides for a range of different outcomes for complaints in NSW. Some of these map to outcomes available under the National Law; others are specific to the NSW jurisdiction. Note that each notification may have more than one outcome; all outcomes have been included.
Notes:
- Includes: Resolved before assessment, Apology, Advice, Council Letter, Comments by Health Care Complaints Commission (HCCC), Deceased, Interview.
- Includes practitioners who failed to renew.
| Current stage of open notification | Less than 3 months | 3–6 months | 6–9 months | 9–12 months | 12–24 months | More than 24 months | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|
| Assessment | 881 | 153 | 52 | 11 | 8 | 5 | 1,110 | 1,079 |
| Health or performance assessment | 79 | 86 | 48 | 29 | 27 | 3 | 272 | 310 |
| Investigation | 564 | 493 | 334 | 331 | 555 | 178 | 2,455 | 2,304 |
| Panel hearing | 8 | 5 | 5 | 1 | 6 | 4 | 29 | 57 |
| Subtotal 2017/18 | 1,532 | 737 | 439 | 372 | 596 | 190 | 3,866 | |
| Subtotal 2016/17 | 1,592 | 716 | 472 | 325 | 555 | 90 | 3,750 | |
| Tribunal hearing1 | 59 | 55 | 69 | 18 | 92 | 28 | 321 | 266 |
| Total 2017/18 | 1,591 | 792 | 508 | 390 | 688 | 218 | 4,187 | |
| Total 2016/17 | 1,641 | 734 | 516 | 364 | 603 | 158 | 4,016 |
Notes:
- Tribunal proceedings are conducted in accordance with timetables set by the responsible tribunal in each jurisdiction.
| Profession | AHPRA1 ACT |
AHPRA1 NSW |
AHPRA1 NT |
AHPRA1 QLD |
AHPRA1 SA |
AHPRA1 TAS |
AHPRA1 VIC |
AHPRA1 WA |
AHPRA1 No PPP2 |
AHPRA Subtotal 2017/18 | HPCA3 | Total 2017/18 | Total 2016/17 | Aboriginal and Torres Strait Islander Health Practitioner | 1 | 1 | 2 | 2 | 2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chinese medicine practitioner | 17 | 2 | 8 | 2 | 29 | 4 | 33 | 29 | |||||
| Chiropractor | 1 | 21 | 7 | 2 | 24 | 22 | 77 | 12 | 89 | 139 | |||
| Dental practitioner | 7 | 11 | 1 | 175 | 18 | 2 | 87 | 49 | 350 | 283 | 633 | 668 | |
| Medical practitioner | 54 | 37 | 35 | 705 | 171 | 58 | 620 | 254 | 14 | 1,948 | 1,355 | 3,303 | 3,080 |
| Medical radiation practitioner | 1 | 2 | 3 | 1 | 8 | 2 | 17 | 6 | 23 | 31 | |||
| Midwife | 5 | 1 | 26 | 6 | 1 | 8 | 7 | 1 | 55 | 21 | 76 | 77 | |
| Nurse | 16 | 11 | 22 | 308 | 166 | 37 | 325 | 120 | 18 | 1,023 | 453 | 1,476 | 1,367 |
| Occupational therapist | 8 | 8 | 1 | 17 | 9 | 26 | 21 | ||||||
| Optometrist | 2 | 8 | 2 | 6 | 2 | 20 | 7 | 27 | 25 | ||||
| Osteopath | 1 | 2 | 5 | 8 | 4 | 12 | 17 | ||||||
| Pharmacist | 5 | 4 | 1 | 74 | 20 | 10 | 98 | 29 | 2 | 243 | 210 | 453 | 399 |
| Physiotherapist | 2 | 3 | 1 | 21 | 10 | 1 | 18 | 7 | 63 | 19 | 82 | 69 | |
| Podiatrist | 3 | 13 | 13 | 6 | 2 | 37 | 9 | 46 | 19 | ||||
| Psychologist | 11 | 5 | 5 | 68 | 29 | 9 | 117 | 53 | 297 | 149 | 446 | 354 | |
| Not identified4 | 1 | 1 | 1 | 1 | |||||||||
| Total 2017/18 | 102 | 77 | 67 | 1,448 | 435 | 121 | 1,345 | 554 | 38 | 4,187 | 2,541 | 6,728 | |
| Total 2016/17 | 107 | 60 | 90 | 1,431 | 492 | 141 | 1,125 | 537 | 33 | 4,016 | 2,282 | 6,298 |
Notes:
- Based on the state and territory of the practitioner's principal place of practice.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- Matters managed by HPCA in NSW.
- Profession of registrant is not always identifiable in the early stages of a notification.
Expanding clinical input
The outcomes of the 2017 Notifications think tank, which looked strategically at how we can improve the notifications process, also included a shared commitment to ensuring robust clinical input is readily available in the management of notifications. In February 2018 a national clinical input service was established to:
- contribute to the reform of our notification process by identifying when and how clinical advice could support better notification management
- develop models for obtaining clinical input from appropriately qualified clinical advisers within the National Scheme specifically suited to different professions based on notification volume
- implement a national process for facilitating health assessments and performance assessments for Part 7 and Part 8 matters across all professions, and
- establish and implement a national process for obtaining independent expert opinions from external providers during investigations.
The aim of this model is to deliver a single clinical input service, accessible to all regulatory staff, with clinical expertise across all professions regulated by the National Scheme. The clinical input service comprises two national teams. The national health and performance assessments team undertakes the administrative processes associated with health and performance assessment coordination. Medical clinical input is provided by a team of clinical advisers: medical practitioners with a diverse range of skills and experience across the medical profession.
The clinical input service will continue to grow in 2018/19 with the extension of clinical input to other professions. While the service will maintain certain profession-specific arrangements, it will ensure a consistent approach to clinical input – particularly in relation to notifications.
Fast-tracking investigations
A direct response to the think tank outcome was to stream lower-risk/lower-complexity matters to be managed by dedicated resources. This outcome was in response to concerns that the lower-risk/lower-complexity matters were often not prioritised because of the demands of other, higher priority investigations.
Fast-track investigation teams were established during January to June 2018 in both Hobart and Darwin to provide services across AHPRA.
Over April to June 2018, the fast-track teams completed a total of 57 investigations, or 7.7% of all investigations completed. The average time these dedicated teams take to complete investigations is less than half the time that more complex investigations take.
The fast-track teams are so far managing matters that are referred to investigation from a triage committee relating to medical and nursing matters. As more professions migrate to new, national intake and assessment processes, there is scope to increase the range of professions whose matters are suitable for management by a fast-track team.
Legal services
AHPRA's regulatory legal services team supports risk-based decision-making and gives advice on policy and procedure across our regulatory functions. The team's primary role is to manage complex or high-risk notifications that progress to a panel or tribunal. It manages appeals and has specialist units handling complaints about alleged statutory offences, release of information and the provision of strategic legal advice.
Tribunals
A National Board can refer a matter to a tribunal for hearing. Usually, this happens with the most serious allegations, such as where the National Board believes a practitioner has behaved in a way that constitutes professional misconduct.
Tribunal proceedings are conducted in accordance with timetables set by the responsible tribunal in each jurisdiction.
The tribunals in each state and territory are:
- New South Wales Civil and Administrative Tribunal
- Australian Capital Territory Civil and Administrative Tribunal
- Northern Territory Civil and Administrative Tribunal
- Queensland Civil and Administrative Tribunal
- South AustralianCivil and Administrative Tribunal
- Tasmania Health Practitioners Tribunal
- Victorian Civil and Administrative Tribunal, and
- Western Australia State Administrative Tribunal.
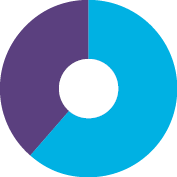
There were 321 notifications open in the tribunal stage as at 30 June 2018, compared with 266 at the same time last year. This increase was anticipated due to multiple years of high rates of notifications. Of the 169 notifications closed by tribunals in the year, 97% of matters resulted in some form of regulatory action or the surrender of registration, while there was a 66.7% reduction in matters resulting in no further action, down to just five individual matters. See Figure 11. This demonstrates that the National Boards' decisions are better identifying the thresholds for referring a matter to a tribunal in order to protect the public.

 97.0% resulted in disciplinary action
97.0% resulted in disciplinary action
 3.0% resulted in no further action
3.0% resulted in no further action
Since 2010, all practitioners who have had their registration cancelled by a court or tribunal, been disqualified from applying for registration, or prohibited from using a specified title or providing a specified health service appear on the cancelled health practitioners register.
We also publish summaries of tribunal outcomes on the Tribunal decisions page on the AHPRA website.
During the year, the Medical Board of Australia started to publish links to disciplinary decisions by courts and tribunals on the public Register of practitioners when there has been an adverse finding about a doctor. The Board decided to introduce links to public tribunal decisions, in the interests of transparency and on the recommendation of the Independent review of the use of chaperones to protect patients in Australia Over the coming year, this approach will also be adopted by other National Boards.
Panels
A National Board has the power to establish two types of panels depending on the type of notification:
- health panels, for issues relating to a practitioner's health and performance, or
- professional standard panels, for conduct and performance issues.
Under the National Law, panels must include members from the relevant health profession as well as community members. All health panels must include a medical practitioner. Each National Board has a list of approved people who may be called upon to sit on a panel.
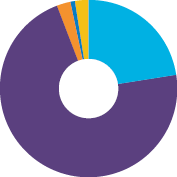
Of the 49 National Board matters decided by panels during the year, more than 75% resulted in some form of regulatory action being taken. See Figure 12.

 32.7% resulted in conditions being imposed or an undertaking being accepted
32.7% resulted in conditions being imposed or an undertaking being accepted
 42.9% resulted in a caution or reprimand
42.9% resulted in a caution or reprimand
 24.5% resulted in no further action
24.5% resulted in no further action
Appeals
All regulatory decisions are evidence-based and guided by the regulatory principles for the National Scheme. The National Law provides a mechanism of appeal against a decision by a National Board in certain circumstances, including decisions to:
- refuse an application for registration or endorsement of registration, or to refuse renewal of registration or renewal of an endorsement of registration
- impose or change a condition placed on registration, or to refuse to change or remove a condition imposed on registration or an undertaking given by a registrant, or
- suspend registration or to reprimand a practitioner.
Decisions may also be judicially reviewed if there is a perceived flaw in the administrative decision-making process, as opposed to a concern about the merits of the individual decision itself.
There were just 28 appeals lodged nationally about decisions made by National Boards under the National Law in 2017/18 (refer to Table 25 and Figure 13). This represents a national reduction of 65.9% when compared with the previous year.
28.6% related to a decision to impose or change a condition on a person's registration or endorsement
28.6% related to a decision to refuse registration, refuse renewal of registration or refuse an endorsement on registration
3.6% related to a decision to refuse to change or remove a condition imposed on a person's registration or the endorsement of a person's registration
 10.7% related to a decision to suspend a person's registration
10.7% related to a decision to suspend a person's registration
 28.6% related to appeals against other decisions
28.6% related to appeals against other decisions
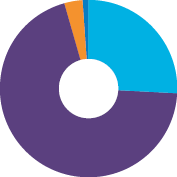
The majority of these appeals related to the professions with higher regulatory decision volumes, such as medical practitioners (13), and nurses (9). There were 71 appeals finalised in 2017/18. Refer to Table 26 and Figure 14.

18.3% had the original decision confirmed
50.7% were withdrawn by the appellant and did not proceed, meaning the original decision remained in place
18.3% resulted in the original decision being substituted with a new decision
(7 matters) or the original decision being amended (6 matters)
12.7% were dismissed on administrative grounds
There were 53 appeals still pending as at 30 June 2018.
The National Scheme's regulatory principles apply to all regulatory decision-making. The principles are designed to encourage a responsive, risk-based approach to regulation across all professions to ensure the public is safe. The low proportion of successful appeals that resulted in an amended/substituted decision demonstrates that the regulatory principles continue to have a positive impact on regulatory decision-making.
More information about appeals in 2017/18 is available in the supplementary tables.
| Profession | AHPRA1 ACT |
AHPRA1 NSW |
AHPRA1 NT |
AHPRA1 QLD |
AHPRA1 SA |
AHPRA1 TAS |
AHPRA1 VIC |
AHPRA1 WA |
AHPRA1 No PPP2 |
AHPRA Subtotal 2017/18 | HPCA3 | Total 2017/18 | Total 2016/17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 0 | 0 | 0 | ||||||||||
| Chinese medicine practitioner | 0 | 1 | 1 | 3 | |||||||||
| Chiropractor | 1 | 1 | 1 | 1 | |||||||||
| Dental practitioner | 1 | 2 | 3 | 3 | 6 | 6 | |||||||
| Medical practitioner | 5 | 1 | 3 | 1 | 1 | 2 | 13 | 13 | 26 | 37 | |||
| Medical radiation practitioner | 1 | 1 | 1 | 1 | |||||||||
| Midwife | 0 | 0 | 0 | ||||||||||
| Nurse | 1 | 1 | 2 | 5 | 9 | 6 | 15 | 26 | |||||
| Nurse and midwife | 0 | 0 | 1 | ||||||||||
| Occupational therapist | 0 | 0 | 0 | ||||||||||
| Optometrist | 0 | 0 | 0 | ||||||||||
| Osteopath | 0 | 0 | 1 | ||||||||||
| Pharmacist | 0 | 0 | 6 | ||||||||||
| Physiotherapist | 0 | 0 | 1 | ||||||||||
| Podiatrist | 0 | 0 | 1 | ||||||||||
| Psychologist | 1 | 1 | 1 | 2 | 6 | ||||||||
| Total 2017/18 | 1 | 7 | 2 | 4 | 6 | 1 | 7 | 0 | 0 | 28 | 24 | 52 | |
| Total 2016/17 | 1 | 9 | 3 | 19 | 10 | 2 | 23 | 14 | 1 | 82 | 8 | 90 |
Notes:
- Based on state and territory of the practitioner's principal place of practice.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- Matters managed by HPCA in NSW.
| Profession | Original decision confirmed – AHPRA1 | Original decision confirmed – HPCA2 | Original decision amended – AHPRA | Original decision amended – HPCA | Original decision substituted for a new decision – AHPRA | Original decision substituted for a new decision – HPCA | Withdrawn – AHPRA | Withdrawn – HPCA | Dismissed – Administrative – AHPRA | Dismissed – Administrative – HPCA | Total 2017/18 – AHPRA | Total 2017/18 – HPCA | Total 2016/17 – AHPRA | Total 2016/17 – HPCA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Appeal against a tribunal decision | 1 | 2 | 1 | 1 | 1 | 2 | 4 | 2 | 0 | |||||
| Decision to impose conditions on a person's registration under section 178 | 3 | 4 | 2 | 16 | 3 | 28 | 0 | 0 | 0 | |||||
| Decision to impose or change a condition on a person's registration or the endorsement of the person's registration | 2 | 2 | 1 | 1 | 1 | 7 | 4 | 2 | 1 | 12 | 9 | 31 | 4 | |
| Decision to refuse to change or remove a condition imposed on the person's registration or the endorsement of the person's registration | 1 | 1 | 1 | 3 | 0 | 5 | 2 | |||||||
| Decision to refuse to endorse a person's registration | 0 | 0 | 1 | 0 | ||||||||||
| Decision to refuse to register a person | 5 | 1 | 9 | 1 | 15 | 1 | 13 | 0 | ||||||
| Decision to refuse to renew a person's registration | 0 | 0 | 3 | 0 | ||||||||||
| Decision to reprimand a person | 0 | 0 | 1 | 1 | ||||||||||
| Decision to suspend a person's registration | 2 | 3 | 3 | 1 | 1 | 5 | 5 | 8 | 6 | |||||
| Other | 0 | 0 | 0 | 1 | ||||||||||
| Not an appellable decision | 1 | 1 | 2 | 0 | 1 | 0 | ||||||||
| Judicial review | 1 | 2 | 1 | 4 | 0 | 3 | 0 | |||||||
| Total 2017/18 | 13 | 7 | 6 | 1 | 7 | 3 | 36 | 5 | 9 | 3 | 71 | 19 | ||
| Total 2016/17 | 11 | 10 | 3 | 0 | 6 | 2 | 44 | 2 | 4 | 0 | 68 | 14 |
Notes:
- AHPRA manages appeals of decisions about NSW registrations.
- Matters managed by HPCA in NSW.
Statutory offences
Performance snapshot
- 581 statutory offence complaints were received this year
- 667 statutory offence complaints were considered and closed
- 189 open statutory offence complaints were still under review as at 30 June 2018, a 48% decrease compared with the previous year
- Over 71% of all new statutory offence complaints related to alleged unlawful use of title and unlawful claims to registration
- 132 new serious-risk advertising complaints were received; 143 were closed
- 13 prosecutions were completed in the Magistrates' or Local Court for statutory offences under the National Law
What are statutory offences?
The National Law includes a number of criminal (summary) offences which relate to conduct that can put individuals and the community at risk. Offences under the National Law may be committed by a person (including registered health practitioners and unregistered individuals) and/or corporate entities. Visit the What is an offence? page on the AHPRA website.
Types of statutory offence
Offences under the National Law predominantly relate to title protection, unlawful claims as to registration, restricted acts, and advertising of regulated health services.
Unlawful use of protected titles
The National Law restricts the use of protected titles (sections 113, 114 and 115). It is unlawful for someone to knowingly or recklessly use a title to make someone believe they are registered in one of the 15 regulated health professions, or other practices including using a specialist title when the person does not have specialist registration or endorsement.
A breach of this type carries a maximum fine of $60,000 for a corporate entity, or $30,000 for an individual, per offence.
Unlawful claims to registrations by individuals or corporate entities
It is unlawful to knowingly or recklessly claim to be a registered health practitioner under the National Law when you do not hold registration (sections 115, 116 and 118). This can include using a title, name, initial, symbol, word or description that could be reasonably understood to indicate that an individual is a health practitioner or is qualified to practise in a health profession. The National Law also states that a person must not claim that another individual is a registered health practitioner.
A breach of this 'holding out' provision is an offence and carries a maximum fine of $60,000 for a corporate entity, or $30,000 for an individual, per offence.
A registered health practitioner must not claim to be a specialist health practitioner if they do not hold registration in the specialist category (sections 117 and 119). A breach of section 117 or 119 by a registered health practitioner does not constitute an offence but may constitute behaviour for which health, conduct or performance action may be taken.
Performing a restricted act
The National Law (sections 121, 122 and 123) restricts certain practices:
- restricted dental acts
- restricted prescription of optical appliances, and
- restricted spinal manipulation.
A breach of restricted act provisions in the National Law carries a maximum fine of $60,000 for a corporate entity, or $30,000 for an individual, per offence.
Unlawful advertising
Under the National Law (section 133), you may not advertise a regulated health service or a business providing a regulated health service in a way that:
- is false, misleading or deceptive or is likely to be misleading or deceptive
- offers a gift, discount or other inducement to attract a person to use the service or the business, unless the advertisement also states the terms and conditions of the offer
- uses a testimonial or purported testimonial about the service or business
- creates an unreasonable expectation of beneficial treatment, or
- directly or indirectly encourages the indiscriminate or unnecessary use of regulated health services.
A breach of the advertising provisions of the National Law is an offence and carries a maximum fine of $10,000 for a corporate entity, or $5,000 for an individual, per offence.
Concerns about unlawful advertising are managed in two ways:
- serious-risk advertising complaints, advertising complaints by corporate entities and unregistered persons are managed as statutory offences, and
- low- to moderate-risk advertising offences by registrants are managed under the Advertising compliance and enforcement strategy.
Statutory offences received and closed in 2017/18
AHPRA recorded 581 new offence complaints during 2017/18.
Most jurisdictions experienced a decrease in offence complaints received when compared with the previous year. Victoria and NSW continue to account for the majority of offence complaints and this year accounted for more than 68% of all new offence complaints.
More than 71% of offence complaints received nationally related to concerns about alleged unlawful use of title and unlawful claims as to registration. See Figure 15.
This year 667 offence complaints have been closed. Refer to Table 27.
As at 30 June 2018, there were 189 statutory offence complaints under review, down from 355 at 30 June 2017, which is a 48% decrease in open offence complaints. See Figure 16.
See Compliance for offence complaints managed under the Advertising compliance and enforcement strategy.
22.7% related to advertising offences by corporate entities or unregistered persons
71.6% related to title protection offences
2.4% related to practice protection offences
0.9% related to directing or inciting unprofessional conduct/professional misconduct
2.4% related to other offences
26.1% related to advertising offences by corporate entities or unregistered persons
69.7% related to title protection offences
3.2% related to practice protection offences
1.0% related to other offences
| Profession | Title protections (s.113–120) – Received | Title protections (s.113–120) – Closed | Practice protections (s.121–123) – Received | Practice protections (s.121–123) – Closed | Advertising breach (s.133) – Received | Advertising breach (s.133) – Closed | Directing or inciting unprofessional conduct/professional misconduct (s.136) – Received | Directing or inciting unprofessional conduct/professional misconduct (s.136) – Closed | Other offence – Received | Other offence – Closed | Total 2017/18 – Received | Total 2017/18 – Closed | Total 2016/17 – Received | Total 2016/17 – Closed |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 1 | 0 | 1 | 3 | 2 | |||||||||
| Chinese medicine practitioner | 19 | 25 | 1 | 2 | 11 | 5 | 31 | 32 | 72 | 38 | ||||
| Chiropractor | 17 | 18 | 2 | 2 | 13 | 10 | 1 | 1 | 33 | 31 | 162 | 192 | ||
| Dental practitioner | 33 | 34 | 8 | 8 | 14 | 14 | 55 | 56 | 239 | 295 | ||||
| Medical practitioner | 114 | 114 | 1 | 1 | 49 | 64 | 5 | 5 | 7 | 7 | 176 | 191 | 273 | 283 |
| Medical radiation practitioner | 6 | 7 | 1 | 1 | 7 | 8 | 4 | 9 | ||||||
| Midwife | 1 | 5 | 1 | 5 | 8 | 35 | ||||||||
| Nurse | 62 | 77 | 2 | 2 | 8 | 9 | 2 | 2 | 74 | 90 | 76 | 80 | ||
| Occupational therapist | 14 | 16 | 14 | 16 | 9 | 13 | ||||||||
| Optometrist | 3 | 2 | 3 | 5 | 6 | 7 | 23 | 24 | ||||||
| Osteopath | 2 | 3 | 2 | 3 | 1 | 1 | 5 | 7 | 252 | 24 | ||||
| Pharmacist | 10 | 14 | 8 | 8 | 1 | 19 | 22 | 53 | 48 | |||||
| Physiotherapist | 28 | 33 | 2 | 8 | 11 | 1 | 1 | 37 | 47 | 940 | 657 | |||
| Podiatrist | 2 | 6 | 2 | 2 | 1 | 1 | 5 | 9 | 20 | 19 | ||||
| Psychologist | 105 | 130 | 1 | 12 | 11 | 3 | 117 | 145 | 116 | 110 | ||||
| Unknown2 | 1 | 1 | 0 | 47 | 56 | |||||||||
| Total 2017/18 | 416 | 485 | 14 | 18 | 1323 | 1433 | 5 | 5 | 14 | 16 | 581 | 667 | ||
| Total 2016/17 | 368 | 422 | 14 | 18 | 1,895 | 1,416 | 6 | 10 | 14 | 19 | 2,297 | 1,885 |
Notes:
- All offences from sections 113–136 of the National Law, not only offences about advertising, title and practice protection.
- AHPRA also received offence complaints about unregistered persons.
- All 2017/18 totals exclude advertising complaints managed entirely through the Advertising compliance and enforcement strategy. These were counted the previous year and are reflected in the 2016/17 totals.
Managing offence complaints
Statutory offences are managed with a risk-based approach, focusing on protecting the public and ensuring the timely resolution of all complaints. All new offence complaints are risk assessed, and this dictates the course of action required to ensure public safety. Offences under the National Law are 'summary offences' and are prosecuted in the Magistrates' or Local Court of the relevant state or territory. All offences under the National Law carry penalties of fines that may be imposed by a Court on a finding of guilt.
As required, serious risk offence complaints are investigated by an inspector. This may include applying to the Magistrates' or Local Court for a warrant to search premises and seize evidence.
AHPRA, in consultation with the relevant National Board, will prosecute offences against individual(s) and/or corporate entities where there is a legitimate public-interest concern to do so.
Advertising requirements
Guidelines for advertising regulated health services have been published to help anyone advertising regulated health services to do so appropriately. In turn, AHPRA and the National Boards have published and implemented an Advertising compliance and enforcement strategy that outlines the risk-based management of offence complaints, particularly advertising complaints.
For more information about the management of low- to moderate-risk advertising complaints, see the compliance section of this report.
Prosecutions under the National Law
There have been a number of significant prosecutions this year that demonstrate the importance of the statutory offence function for the protection of the public.
AHPRA completed 13 proceedings in the Magistrates' and Local Courts for offences under the National Law across three jurisdictions. All prosecutions resulted in findings of guilt; eight with a conviction and five with no conviction recorded; and in all cases the individual or entity was fined. These outcomes demonstrate that AHPRA continues to identify appropriate thresholds for referring offence complaints for prosecution to protect the public.
Further information about these matters is outlined in Table 28 and Figure 17. Some prosecutions that started in 2017/18 and were concluded after the financial year have been reported here for completeness. Information about AHPRA's prosecutions is available on the News page on the AHPRA website.
A further six prosecutions are ongoing before the courts as at 30 June 2018.
61.5% resulted in a conviction recorded against the individual, and an order to pay a fine and/or complete a period of community service or good behaviour
38.5% resulted in a finding of guilt with 'no conviction recorded', but the individuals were still ordered to pay a fine and/or complete a period of community service or good behaviour
| Defendant | Date of decision | Jurisdiction | Relevant Board | Relevant section of National Law1 | Type of offence | Outcome | Sentence |
|---|---|---|---|---|---|---|---|
| De-identified2 | 29 August 2017 | Vic | NMBA | s. 113(1)(a), s. 116(1)(b)(i), s. 116(1)(c) |
|
Found guilty but no conviction recorded | The accused was fined $6,000 and ordered to pay costs of $8,217. |
| Jangodaz, Reza | 11 September 2017 | NSW | DBA | s. 116(1)(c) |
|
Convicted | The accused was fined $4,750 and ordered to pay costs of $4,000. |
| De-identified | 27 September 2017 | Vic | MBA and PsyBA | s. 113(1)(a), s. 116(1)(c), s. 118(1)(b)(ii), s. 118(1)(c) |
|
Found guilty, but no conviction recorded | The accused was fined $20,000 and ordered to pay costs of $10,000. |
| Wellness Enterprises Pty Ltd t/a Australian Male Hormone Clinic | 3 October 2017 | Vic | MBA | s. 133(1)(d) |
|
Convicted | The accused was fined $127,500 ($7,500 per offence) and ordered to pay costs of $6,000. |
| Morris, Chantelle | 17 November 2017 | Qld | NMBA | s. 113(1), s. 116(1)(c) |
|
Convicted | The accused was fined $12,000 and ordered to pay costs of $3,916. |
| De-identified | 25 January 2018 | Vic | PsyBA | s. 113(1)(a), s. 116(1)(b)(i), s. 116(1)(c) |
|
Found guilty, but no conviction recorded | The accused was fined $4,500 and ordered to pay costs of $7,500. |
| Zaphir, George | 30 January 2018 | Qld | ChiroBA | s. 113(1)(a), s. 116(1)(b), s.116(1)(c) |
|
Convicted | The accused was fined $12,000 and ordered to pay costs of $3,537. |
| Mohamad Anwar, Mohamad Faizal | 1 February 2018 | Vic | MBA | s. 116(1)(c) |
|
Convicted | The accused was fined $100,000 ($25,000 per offence) and ordered to pay costs of $14,885. |
| De-identified | 5 February 2018 | Vic | PsyBA | s. 113(1)(a), s. 116(1)(c) |
|
Found guilty, but no conviction recorded | The accused was fined $10,000 and ordered to pay costs of $14,325. |
| De-identified | 6 February 2018 | Vic | MBA | s. 116(1)(c) |
|
Found guilty, but no conviction recorded | The accused was fined $7,500 and ordered to pay costs of $20,000. |
| Be, Karren | 28 February 2018 | NSW | PharmBA | s. 113(1)(a) (withdrawn), s. 116(1)(c) |
|
Conviction | The accused was fined $11,250 and ordered to pay costs of $6,920. |
| Citer, David | 9 May 2018 | NSW | PsyBA | s. 116(1)(b)(ii) |
|
Conviction | The accused was fined $9,500 and ordered to pay costs of $5,000. |
| Lipohar, Edward | 7 June 2018 | Vic | DBA | s. 118(1)(c), s. 121(1) |
|
Conviction | The accused was fined $65,000 and ordered to pay costs of $25,000. The fine and cost order stayed for six months on application of the accused. |
Notes:
- The Health Practitioner Regulation National Law, as in force in each state and territory.
- Prosecutions are de-identified when the court makes a finding of guilt with 'no conviction recorded' or a spent conviction, or when the charges are withdrawn. Cases may also be de-identified where the court grants a suppression order.
Compliance
Performance snapshot
- 5,065 cases were being actively monitored by AHPRA at 30 June 18 – these cases related to 5,005 registered practitioners
- 27.6% were about conduct, health or performance
- 66.1% were about suitability/eligibility for registration
- 6.2% related to prohibited practitioners/students
- As at 30 June 2018, there were 70 restrictions (conditions or undertakings) in the National restrictions library
- 911 new low- to moderate-risk advertising complaints about registrants were managed under the Advertising compliance and enforcement strategy
How AHPRA monitors compliance
On behalf of the National Boards, AHPRA monitors health practitioners and students with restrictions (conditions or undertakings) placed on their registration, as well as those with suspended or cancelled registration. By identifying any non-compliance with restrictions and acting swiftly and appropriately, AHPRA supports Boards to manage risk to public safety.
To find out about active monitoring cases in 2017/18, please refer to Tables 29 and 30. Table 29 reports on active monitoring cases by state and territory. Table 30 reports on these cases by each profession. Restrictions are placed on a practitioner's registration through a number of mechanisms, including as an outcome of a notification, or when a practitioner applies for registration or renewal of registration.
Each monitoring case is assigned to one of five streams.
A practitioner or student is being monitored because they have a physical or mental impairment, disability, condition or disorder (including substance abuse or dependence).
A practitioner is being monitored to ensure they practise safely and appropriately while demonstrated deficiencies in their knowledge, skill, judgement or care in the practice of their profession are addressed.
A practitioner is being monitored to ensure they practise safely and appropriately following consideration of their criminal history, or they have demonstrated a lesser standard of professional conduct than expected.
A practitioner is being monitored because they:
- do not hold an approved or substantially equivalent qualification in the profession
- lack the required competence in the English language, or
- do not meet the requirements for recency of practice, or do not fully meet the requirements of any other approved registration standard.
A practitioner or student is being monitored because they:
- are subject to a cancellation order, suspension or restriction not to practise, or
- have surrendered registration or changed to non-practising registration, in lieu of further action, under Part 8 of the National Law or suspension.
This year, the number of active monitoring cases nationally decreased by 0.4%. The cases monitored by AHPRA relate to 5,005 individual practitioners and the majority were in relation to monitoring of eligibility/suitability requirements. There was also a 23.0% (59 cases) increase in the number of cases relating to a prohibited practitioner/student when compared with last year.
Expanding our reporting capability
Since the introduction of compliance performance reporting in 2015/16, we have continued our focus on managing risks associated with monitoring cases and identifying opportunities to improve the quality, timeliness and accuracy of our compliance work, including in reporting. Improvements have been made to our ability to report at the level of restriction categories for each compliance case. Reporting at restriction level has many advantages for understanding risks associated with the monitoring of each individual practitioner and the overall monitoring caseload. These improvements will:
- provide a simple and efficient tool to extract information about how many registrants are subject to monitoring for particular types of restrictions, such as for boundary violations, drug and alcohol testing, education and up-skilling, practice limitations and supervised practice
- provide a simple and efficient tool to extract reports about how many practitioners are subject to monitoring for 1, 2, 3, 4, 5 or more concurrent restriction categories, and
- enable the development of more effective mechanisms for identifying the complexity of monitoring cases, for establishing the resources required to monitor particular cases and for the management of individual and team caseloads.
Performance has remained strong across all key performance indicators in all quarters.
Advertising compliance and enforcement
AHPRA's compliance and legal divisions manage the enforcement aspects of the Advertising compliance and enforcement strategy. We have established an advertising compliance team, which is responsible for the triaging of all offence complaints, the assessment of all advertising offence complaints and the ongoing management of low- and moderate-risk advertising complaints under this strategy.
The strategy was developed to ensure advertising about regulated health services is done responsibly to keep the public safe from false or misleading claims and to help them make informed choices about their healthcare. It explains how:
- our risk-based approach is applied to advertising compliance and enforcement
- we encourage voluntary compliance and deal with non-compliant advertising, and
- we plan to evaluate and refine this strategy.
Responsible advertising is a professional and legal obligation. We recognise that most health practitioners want to comply with the law and their professional obligations, and we aim to make compliance as easy as possible.
The data in 2017/18 confirm that nearly 50% of registrants become compliant in response to the initial letter about the advertising breach, with the remainder becoming compliant when the imposition of advertising restrictions is being considered and the practitioner is issued with the show cause notice where each breach and its location is specified. This demonstrates the effectiveness of the strategy in educating practitioners on their professional obligations and ensuring timely remediation of inappropriate advertising for the benefit of the public. There were no instances of continued non-compliant advertising that required regulatory action through the imposition of advertising restrictions.
You can read the Advertising compliance and enforcement strategy on the AHPRA website.
Counselling restrictions pilot
This year, National Boards endorsed the introduction of counselling as a notifications outcome by placing a restriction on a practitioner's registration requiring the practitioner to attend Board-led counselling. This is only done in conjunction with a formal caution and to reinforce the issues and reasons for the caution with the practitioner and explore what is required of the practitioner to improve their conduct to prevent recurrence of the issues.
National Boards also endorsed the concept of a pilot with the Psychology Board of Australia to review and confirm the decision-making considerations for imposing a counselling restriction, Board member training, the monitoring process and the overall impact on the practitioner's insights into past conduct and prevention strategies.
The implementation of the pilot was supported by the compliance function, primarily through:
- drafting of policy and guidelines to support the use of a counselling restriction
- development of a standard counselling restriction for use in the pilot
- revising template notices to include an information sheet on the counselling process
- developing and implementing processes to support the policy position and the actual counselling requirement, and
- developing and implementing Board member training on decision-making considerations for imposing a counselling restriction, appointment of counsellors, conducting the counselling and record-keeping associated with the counselling requirement.
The pilot outcomes will inform the wider use of counselling restrictions across all professions.
| AHPRA ACT |
AHPRA NSW1 |
AHPRA NT |
AHPRA QLD |
AHPRA SA |
AHPRA TAS |
AHPRA VIC |
AHPRA WA |
AHPRA No PPP2 |
AHPRA Subtotal 2017/183 | HPCA4 | Total 2017/18 | Total 2016/17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Conduct | 7 | 3 | 5 | 52 | 45 | 10 | 107 | 44 | 2 | 275 | 365 | 640 | 687 |
| Health | 14 | 11 | 12 | 251 | 58 | 20 | 114 | 71 | 13 | 564 | 320 | 884 | 896 |
| Performance | 14 | 6 | 14 | 143 | 75 | 23 | 198 | 85 | 3 | 561 | 166 | 727 | 684 |
| Prohibited practitioner/student | 3 | 3 | 10 | 55 | 58 | 9 | 131 | 42 | 4 | 315 | 315 | 256 | |
| Suitability/eligibility5 | 52 | 1,292 | 40 | 544 | 224 | 41 | 628 | 415 | 114 | 3,350 | 3,350 | 3,343 | |
| Total 2017/18 | 90 | 1,315 | 81 | 1,045 | 460 | 103 | 1,178 | 657 | 136 | 5,065 | 851 | 5,916 | |
| Total 2016/17 | 113 | 1,353 | 53 | 1,069 | 450 | 107 | 1,138 | 666 | 135 | 5,084 | 782 | 5,866 |
Notes:
- Includes cases to be transitioned from AHPRA to HPCA for conduct, health and performance streams.
- No principal place of practice (No PPP) includes practitioners with an overseas or unknown address.
- It should be noted that the AHPRA data structure provides reports by monitoring cases established rather than by registrants being monitored. This is because a registrant may have a set of restrictions (conditions or undertakings) in more than one stream. For 2017/18, the 5,065 AHPRA monitoring cases relate to 5,005 registrants (distinct registrants per profession). The data provided by HPCA report the number of registrants being monitored.
- HPCA monitors conduct in relation to health, performance and conduct in NSW.
- AHPRA performs monitoring of compliance cases in 'suitability/eligibility' matters for NSW registrations.
| Profession | Conduct – AHPRA |
Conduct – HPCA |
Health – AHPRA |
Health – HPCA |
Performance – AHPRA |
Performance – HPCA |
Prohibited practitioner/student – AHPRA |
Suitability/eligibility1 – AHPRA |
Total 2017/18 – AHPRA2 |
Total 2017/18 – HPCA |
Total 2016/17 – AHPRA2 |
Total 2016/17 – HPCA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Practitioner | 4 | 2 | 1 | 55 | 62 | 0 | 72 | 0 | ||||
| Chinese medicine practitioner | 5 | 1 | 4 | 1 | 2 | 876 | 887 | 2 | 945 | 2 | ||
| Chiropractor | 6 | 4 | 4 | 3 | 8 | 6 | 16 | 40 | 7 | 49 | 9 | |
| Dental practitioner | 12 | 23 | 17 | 13 | 66 | 50 | 6 | 22 | 123 | 86 | 134 | 60 |
| Medical practitioner | 100 | 192 | 205 | 125 | 230 | 29 | 85 | 1,072 | 1,692 | 346 | 1,620 | 340 |
| Medical radiation practitioner | 1 | 6 | 2 | 4 | 2 | 95 | 108 | 2 | 88 | 3 | ||
| Midwife | 3 | 1 | 4 | 1 | 9 | 2 | 137 | 155 | 2 | 155 | 2 | |
| Nurse | 85 | 66 | 281 | 146 | 161 | 63 | 178 | 818 | 1,523 | 275 | 1,553 | 251 |
| Occupational therapist | 1 | 4 | 1 | 1 | 52 | 57 | 2 | 51 | 4 | |||
| Optometrist | 2 | 1 | 2 | 6 | 1 | 12 | 22 | 2 | 15 | 1 | ||
| Osteopath | 1 | 1 | 1 | 3 | 1 | 4 | 9 | 2 | 6 | 4 | ||
| Pharmacist | 17 | 61 | 19 | 14 | 32 | 12 | 11 | 93 | 172 | 87 | 175 | 76 |
| Physiotherapist | 9 | 3 | 3 | 3 | 10 | 2 | 3 | 33 | 58 | 8 | 64 | 3 |
| Podiatrist | 3 | 3 | 1 | 1 | 10 | 17 | 1 | 14 | 0 | |||
| Psychologist | 35 | 12 | 12 | 10 | 23 | 7 | 15 | 55 | 140 | 29 | 143 | 27 |
| Total 2017/18 | 275 | 365 | 564 | 320 | 561 | 166 | 315 | 3,350 | 5,065 | 851 | ||
| Total 2016/17 | 356 | 331 | 577 | 319 | 552 | 132 | 256 | 3,343 | 5,084 | 782 |
Notes:
- AHPRA performs monitoring of compliance cases in 'suitability/eligibility' matters for NSW registrations.
- It should be noted that the AHPRA data structure provides reports by monitoring case established rather than by registrants being monitored. This is because a registrant may have a set of restrictions (conditions or undertakings) in more than one stream. For 2017/18, the 5,065 AHPRA monitoring cases relate to 5,005 registrants (distinct registrants per profession). The data provided by HPCA report the number of registrants being monitored.